By Tom Lawry
•
February 24, 2026
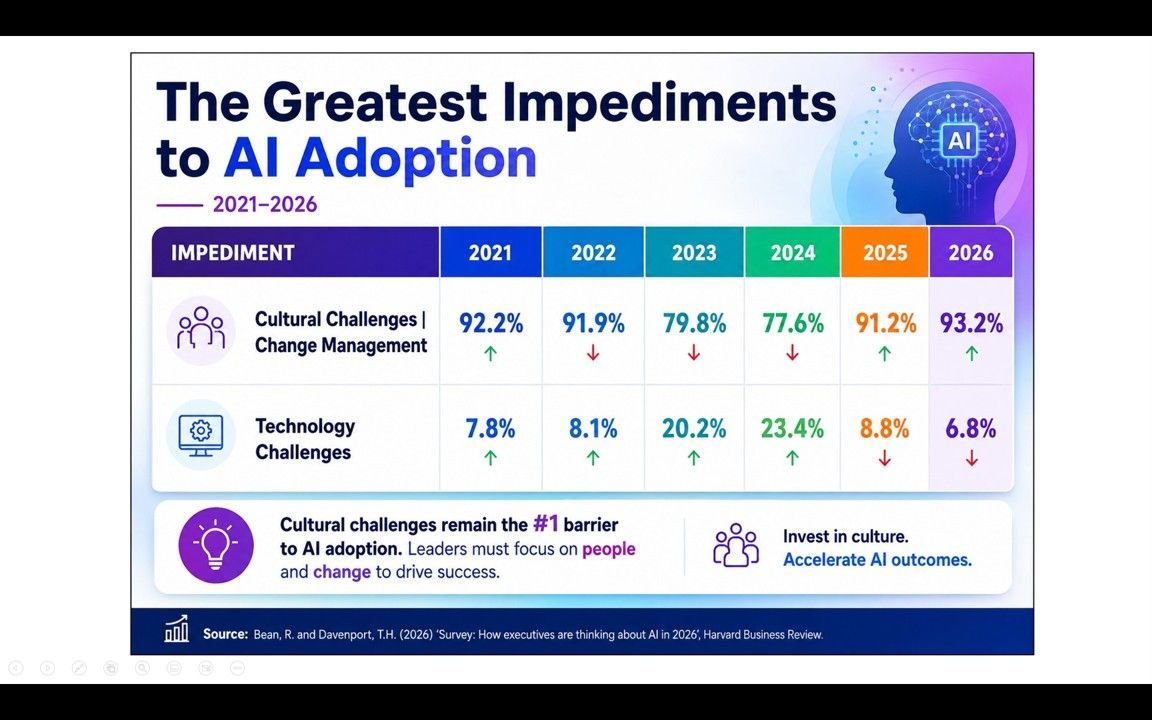
We've reached a strange paradox in healthcare: AI adoption is accelerating, investment is growing, and vendor solutions are multiplying — yet most organizations are not seeing AI value actually scale across clinical outcomes, financial performance, or operations. I see this pattern constantly. Healthcare is good at starting AI. We are far less good at turning it into something that measurably and consistently changes results for the people we serve. Here are the five reasons I see most often, and one overlooked leadership skill that, when present, dramatically increases the odds of success. Five Reasons AI Value Stays Locked 1. No clear definition of value — before you start In my experience, many organizations deploy AI without first agreeing on what success looks like in measurable terms. Metrics are vague, retrospective, or disconnected from clinical or financial performance. Without a pre-defined baseline and agreed-upon KPIs, there's no way to demonstrate ROI — and initiatives drift without accountability. Projects get declared "complete" at go-live, not at value realization. 2. Pilots that go nowhere Healthcare is highly adept at piloting AI. Industrializing it is another story. I've watched impressive pilots stall out more times than I can count — and the data backs this up: only about 30% of AI healthcare pilots make it to full production. Most are siloed experiments with no integration into operational workflows, no change management plan, and no budget for enterprise rollout. The result is a graveyard of promising ideas that never escape proof-of-concept. Value locked in pilots cannot move system-level metrics. 3. Data that isn't ready AI performs only as well as the data it consumes. In healthcare, that data is fragmented across EHR systems, legacy platforms, and departmental silos — with inconsistent coding, missing fields, and poor interoperability. Where data does exist, governance structures around quality, access, and lineage are often immature. The result is models that underperform, eroding the clinical trust that adoption depends on. 4. Change management treated as an afterthought This one frustrates me most. AI implementation is too often treated as a technology project rather than a people and process transformation. Insufficient time and resources go toward training end users, redesigning workflows, and building the clinical and operational champions needed to sustain adoption. Without behavioral change, technology plateaus well below its potential — or simply goes unused. 5. AI chasing the wrong priorities Many AI investments I see are driven by vendor marketing, peer benchmarking, or departmental enthusiasm rather than enterprise strategic need. The result is a portfolio of capabilities that don't address what leadership is actually accountable for: cost reduction, quality metrics, patient access, margin improvement. Optimizing the wrong things produces activity, not outcomes. The Real Problem Isn't the Technology Here's what I've come to believe after working through these challenges with many organizations: the AI tools available today are genuinely capable of driving meaningful outcomes. The failure points are structural, organizational, and strategic — rooted not in how algorithms work, but in how leaders plan, deploy, govern, and evaluate. The single most important thing I've learned about scaling AI innovation is this: innovation is a voluntary act. You cannot force people to embrace something new. You can only create the conditions that make them want to. The Hidden Leadership Skill: Become a Bridger This is where a framework I recently encountered has genuinely shifted how I think about the problem. In their new book Genius at Scale, Linda A. Hill, Emily Tedards, and colleagues introduce what I consider one of the most useful concepts for scaling innovation I've come across. They call it "Bridging" — and the leaders who do it well, they call "Bridgers." Bridgers are not the loudest voices in the room. They are not necessarily the most technical. What makes them disproportionately effective is their ability to work at the intersection of people, trust, and collaboration across organizational boundaries. In practice, I see this play out in three ways: Bridgers curate the right partners. They are deliberate about who needs to be at the table — not just the technology team or the clinical champions, but operational leaders, finance partners, and the frontline staff whose workflows will actually change. And they bring these people in early, before decisions are made. Bridgers build mutual trust. They listen more than they advocate. They communicate upward, downward, and laterally. What I find most powerful here is their understanding that persuading someone to embrace a new idea requires understanding not just what they say — but what they value, what they fear, and what's already weighing on them when they show up to work. Bridgers create mutual commitment. They don't hand off and move on. They stay engaged through implementation, through the hard middle, through the moments when adoption stalls and the metrics aren't moving yet. They hold coalitions together when momentum fades. When I step back and look at the organizations that are actually scaling AI value, this is what I see in common. It's not the most sophisticated technology stack. It's not the biggest budget. It's leaders who understand that done right, AI in healthcare isn't fundamentally about technology — it's about empowerment. Helping clinicians be better at what they care about. Giving operational leaders clearer signal through the noise. Helping mission-driven organizations learn faster than their problems are growing. Leaders who embrace this won't just deploy AI. They'll scale it into something that genuinely changes what their organizations can do. The question I keep coming back to is a simple one: Who in your organization is playing the Bridger role right now?